|
In this method, the patient is
asked about the intake of food on a normal day. Each intake is related
to the patient's habits and social situation, for example, the morning
meal, the consumption in the trip to work, snacks between meals and
snacks during work. Try to understand why certain articles seem
necessary and aim to correct said diet scheme.
One way to do it is through the following diet
story:
-
Breakfast: What do you
drink and what do you eat?
Sugar: How much?
-
What do you drink, eat
or chew between breakfast and lunch?
Sugar: How much?
-
Lunch: What do you
drink and what do you eat?
Sugar: How much?
-
What do you drink, eat
or chew between lunch and snack?
Sugar: How much?
-
Snack: What do you
drink and what do you eat?
Sugar: How much?
-
What do you drink, eat
or chew between your snack and dinner?
Sugar: How much?
-
Dinner: What do you
drink and what do you eat?
Sugar: How much?
-
What do you drink, eat
or chew after dinner and before going to bed?
Sugar: How much?
Brush your teeth before going to bed?
-
What do you drink, eat
or chew during the night if you wake up?
Sugar: How much?
The premise of this survey is to reduce the
daily frequency of food intake containing fermentable
carbohydrates (sugar). Frequency is called the number of times
the patient eats the food rich in sugar on the day (24 hours).
This is also known as sugar moment.
The questions in the questionnaire determine the
amount of food the patient eats between meals (snacks). If you answer
all of these questions that you eat certain food that has sugar, our
patient has more than 5 sugar moments between meals (24 hours). risk of
having new cavities.
Then you should eliminate sugar from snacks or
snacks: "Snacks between meals containing sugar
should be less than 3 in 24 hours"
- You can substitute snacks with sugar for
snacks with sweeteners. (low calories, sugar free)
- You can eliminate sugar snacks from your
daily diet, but so that you do not have an appetite between meals,
you should have the four most substantial central meals of the day.
The professional must understand that a healthy
diet is difficult to accept by our patients. They do not usually
associate the risk of caries with fermentable carbohydrates (sugar).
Only the repetition of the information, about the healthy diet and its
future benefits, can change a nutritional habit.
A low sugar intake is desirable from a
karyological point of view. (SIGN 1 ++, GRADE A) 57
A low frequency of sugar is desirable from a
cariological point of view. According to WHO studies, "Caries in
children does not happen when the consumption of national sugar is below
10 kg per capita per year, or about 30 grams per day, but an increase of
15 kg produces a significant increase in tooth decay" (220) On the other
hand, with effective preventive programs it is possible to increase the
consumption of sugar, without producing an increase in caries. (see, for
example, the relationship between the consumption of sugar and cavities
in Iceland on the WHO Oral Health Country Profile Program website).
The problem of the concentration of carbohydrates,
sugar in relation to caries is complex. Experimental studies have shown
that there is a correlation between carbohydrate intake and enamel
demineralization (221). Also, a high glucose concentration hinders the
natural protective mechanism of the mouth (222). In this study, rinsings
were performed with different concentrations of glucose, from 0.3% to
50%. The 0.3 and 0.5% mouthwashes were removed from the oral cavity in a
time of 3 minutes, while the 50% glucose mouthwashes were eliminated in
a longer period, approximately 27 minutes.
On the other hand, there is no increase in plaque,
but low pH of the plaque is prolonged over time. The different
concentration of carbohydrates in the meals plays an important role for
the development of caries. (223)
Carbohydrates are the main energy source for oral
bacteria and can reduce the pH of the critical level. Some carbohydrates
are of particular interest:
|
Fermentable
carbohydrates
|
|
Carbohydrates |
Chemical
form |
Bacterial
metabolism (Streptococcus mutans) |
Cariogenicity |
|
Metabolic
process |
Final
metabolic product |
|
Glucose
|
Hexose |
Anaerobic glycolysis
|
Lactic acid
|
+
|
|
Fructose
|
Hexose |
Anaerobic glycolysis
|
Lactic acid
|
+
|
|
Starch
|
Glucose polymer (C 1-4 bond) |
Degradation by amylase (glucose)
|
Glucose - Lactic acid
|
+
|
|
Cellulose
|
Glucose polymer (B 1-4 bond) |
None
|
None
|
-
|
|
Saccharose (sugar)
|
Disaccharide of the most
fructose glucose (bond 1-2) |
Glucolysis + Synthesis of
extracellular polysaccharides. Synthesis of intracellular
polysaccharides.
|
Lactic acid + extracellular
glucan or extracellular fructan + extracellular amylopectin. |
++++
|
The use of sugar substitutes
results in a low production of acids.
To reduce the risk of dental
caries, great efforts have been made to find suitable substitutes
for sucrose. The advantages of these compounds have to be evaluated
in several aspects that include nutrition, toxicology and technical
aspects. Sucrose substitutes can be divided into two main categories:
caloric and non-caloric sweeteners.
Caloric sweeteners consist of sugars and sugar alcohols. These
products contain calories like sucrose. Sugars such as glucose,
fructose and invert sugar are mainly used in processed foods for
babies. The acid production in dental plaque is however equal to
that of sucrose. Despite this, these sugars are considered less
cariogenic than sucrose; because they produce less amounts of plaque
(226)
Non-caloric sweeteners are
chemically a very heterogeneous group. All of them have in common an
intense sweet taste and do not contain enough energy. They can not
be metabolized by oral bacteria, aspartame, cyclamate and saccharin.
They are perfect to avoid the process of decay, but they have some
disadvantages: taste, stability and lack of volume. (227)
Xylitol: Xylitol is quite
expensive, it is used in chewing gum, saliva substitutes,
toothpastes, fluoride tablets, etc. Many studies have shown that
xylitol can be considered non-cariogenic and can also have an
antimicrobial effect, because less accumulation of dental plaque has
been observed after consumption.
Xylitol is a penta alcohol found
naturally in a variety of fruits and vegetables (raspberries,
strawberries, plums, lettuce, cauliflower, mushrooms, sorghums) and
is obtained commercially from birch trees, seed husks of cotton, and
coconut shells. It has a sweetness similar to sucrose and a
refreshing effect in the mouth. It has been proposed as a possible
sugar substitute for diabetic patients, although in high doses it
can cause diarrhea in humans and rats.
In Turcu, Finland, studies have
been carried out in a population with an average age of 27, 5 years,
where one group consumed sucrose, another was fructose and another
group consumed xylitol. These are the conclusions;
-
After two years the
Xylitol group had a 90% less incidence of caries than the
group that consumed sucrose.
-
The Fructose group only
had 25% less caries than the sucrose group.
-
The amount of dental
plaque was reduced by 50% in the Xylitol group compared to
the sucrose group.
Xylitol produced a significant reduction of Candida albicans
(approximately 60-70%).
-
One year after the study
ended the amount of S. mutans was still significantly low in
the Xylitol group.
-
A significant caries
reduction was found in the Xylitol group, and a lower
reduction in the Fructose group compared to the Sucrose
group.
The O'Leary index is used to
evaluate the hygiene of smooth surfaces. Indicates the percentage of
smooth stained surfaces (in pink and blue, if double tone is used)
on the total of dental surfaces present. The patient should perform
a crop with water to remove excess dye. Preferably the double tone
should be used, since this developer can see the mature Bactrian
plate in dark blue color, which is considered cariogenic and
periodontopathic; and the plate of less than 24 hours, considered
bacterial plaque of the day in pink.
This index is applied at the
initial moment and throughout the treatment to determine the ability
to control the plaque with daily toothbrushing, before and after
teaching oral hygiene. And it is obtained by applying the following
formula.
|
|
|
Number of stained surfaces X 100 =
|
|
Total surfaces present
|
Each tooth is considered constituted by
four surfaces. The registration to determine the O'Leary index is done
by marking the stained surface on the ad hoc diagrams.
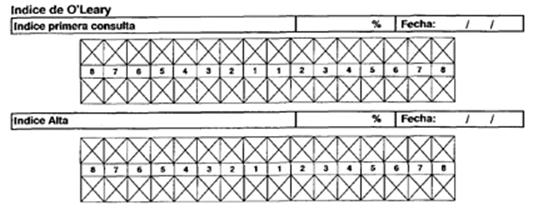
Optimal value of the
O'Leary index <= 20%
The O'Leary index is mandatory in the first
consultation, since it is based on the principle of self-care on the
part of our patient. The complement of the O`Leary index is the occlusal
plaque index.
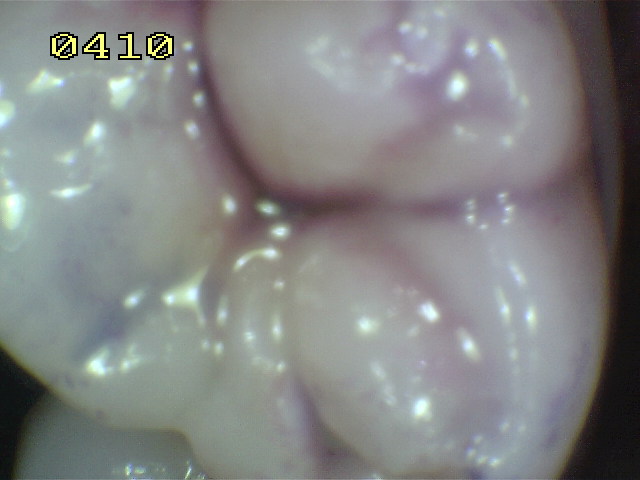
The occlusal plaque index is used to
evaluate the hygiene of the occlusal surfaces. For this, a revealing
solution of bacterial plaque (double tone) is used. The patient should
rinse with water to remove excess dye. The following table shows the
criteria used.
|
Occlusal plaque index |
|
0 |
No bacterial plaque. |
|
1 |
Pink bacterial plaque in pits and
fissures. |
|
2 |
Pink bacterial plaque in pits
and fissures, with blue islets |
|
3 |
Blue bacterial plaque in pits and
fissures. |
|
|
|